Neuro Landscape
A Brain Injury Blog by Centre for Neuro Skills

(Note: This is a guest blog from Brent E. Masel, M.D, the Executive Vice-President for Medical Affairs for CNS and a Clinical Professor of Neurology at the University of Texas Medical Branch in Galveston. In this article, Dr. Masel addresses the increasing rate of strokes in young people).
As is well known, stroke is one of the leading causes of disability and death in the United States. We all assume this is a problem of the elderly. For the most part, it is; nevertheless, it is increasingly becoming a significant problem in the younger population.
Interestingly, the incidence of strokes in the US amongst patients older than 65 years has decreased over the past few decades. Population studies, however, have shown an increase in strokes in young adults. Nationally, approximately 11% of strokes occur in young adults.
We are now seeing an increased prevalence of traditional cardiovascular risk factors in adults aged 18 to 64. The prevalence of three or more conventional risk factors such as hypertension, elevated cholesterol, tobacco use, and obesity has nearly doubled in young adults when compared to older populations. Additional “lifestyle diseases” that increase the risk for stroke include substance abuse such as cocaine and possibly cannabis. Cervical artery dissection (tearing of the carotid artery in the neck), usually caused by trauma to the neck is an essential cause of stroke in the young adult population.
Migraine may be a cause of stroke in a large percentage of patients, especially those with well-defined premonitory symptoms. The risk of stroke in women with migraines is especially increased in those who are heavy smokers. Oral contraceptive use has long been known to be a possible cause of stroke in young females, again, with an increased risk with heavy smoking.
It should also be noted that despite a comprehensive evaluation, in a considerable portion of young stroke patients, no clear cause is found.
A stroke in a young adult carries a significant risk for post-stroke complications. A Dutch study showed that the risk of mortality is four times higher in young patients who have strokes compared to those who don’t. Post-stroke depression is common at all ages and is undoubtedly very important in the young. It also may be related to increased mortality in the young adult population. Other factors that may contribute to a poor outcome include post-stroke pain, cognitive deficits, fatigue, and sexual dysfunction.
Children are not immune to strokes. An extensive survey in the United States found an incidence of stroke of .58 per 100,000 children aged 1 to 14 years. The most common causes were blood vessel disease and sickle-cell disease. Approximately 17% of children with sickle cell disease will have a clinically silent stroke as detected by MRI. 10%-15% of children with sickle cell disease will have a stroke by age 20. Sickle cell disease, therefore, is an important potentially preventable cause of stroke in children and young adults.
Interestingly, a chickenpox infection in the preceding year was noted in 31% of children aged 6 months to 10 years who had a stroke compared to a 9% rate in the general population. The risk of chickenpox associated stroke is estimated to be one in 15,000 children.
So what can the reader take away from this blog?
Strokes in the young adult population are on the rise even though it is decreasing and the older adult population. To a great extent, many of the risks of having such an unfortunate event can be modified by lifestyle changes. We encourage the readers of this blog to take inventory of their lifestyle choices and take control of their health.
(Note: In this guest blog from Grace Griesbach, Ph.D., and CNS’ National Director of Clinical Research, she explains that proper sleep is a vital component in the rehabilitation of brain injury).
Historically, quotes referring to sleep have been associated with well-being. This is not without substance. The importance of sleep is appreciated when one considers that it is observed across the vast majority of animal species. In humans and other higher mammals, lack of sleep has been demonstrated to impact physical, cognitive and emotional functions negatively. Physical consequences of sleep deprivation include compromised immune responses, as well as hormonal and metabolic alterations that in turn will impact overall health. Sleep also promotes emotional and psychological well-being. As for cognitive functions, sleep has been shown to facilitate learning and memory.
Moreover, animal studies have shown that neural plasticity changes allow for better memory to occur during sleep. Sleep driven neural plasticity is also evident during brain development and during times when healing is necessary. Given the multiple functions of sleep, it is evident that sleep-related problems should not be ignored.
Unfortunately, the prevalence of sleep disorders following brain injury is notably higher compared to the general population. Many of those that have endured a traumatic brain injury or stroke have difficulty initiating or maintaining sleep. Daytime sleepiness (hypersomnia) and fatigue are frequently reported complaints that are associated with insomnia. Apnea, a common breathing-related sleep disorder, is frequently observed during the chronic brain injury period. Apnea is defined as breathing cessation for fixed periods during sleep and contributes to arousals throughout the night; promoting fragmented sleep.
Sleep follows a particular overnight pattern consisting of repeated sleep cycles. Each cycle is comprised of one rapid eye movement (REM) stage and three non-REM stages. These stages are defined by different brain activity patterns that have been associated with particular physiological and neural plasticity processes.
Studies focused on proper sleep closely examine brain wave activity and body physiology throughout the various sleep stages. Some stages are particularly important for memory, emotional well-being, and cognitive function, and may be compromised by interrupted sleep. The golden standard of evaluating sleep is with an overnight polysomnography study performed by a certified sleep technologist. The technologist places electrodes on the scalp of the patient to record brain activity. Breathing, heart rate, oxygen levels, and limb movement are also recorded during sleep. Results from these recordings are sent to a board-certified sleep medicine physician, who creates a report on the diagnosis and a treatment plan.
Centre for Neuro Skills (CNS) offers a comprehensive multidisciplinary approach to rehabilitation. This entails addressing key factors that impact recovery such as sleep. CNS has opened sleep laboratories within the residential buildings of our programs in Dallas, Texas and Bakersfield, California. All CNS facilities can arrange for a sleep evaluation at one of the labs, based on a patient’s needs and treatment plan. Sleep evaluations of CNS patients allow for the detection of sleep-related issues that are likely to hinder recovery. CNS sleep facilities also provide research opportunities to deepen understanding of sleep-related issues after brain injury. Findings from these studies will help improve treatment and develop new therapeutic strategies.
(Note: This is part two of a two-part series on issues affecting worker’s compensation, brain injury rehabilitation, and appropriate patient care).
The focus in health care today is often on the high cost of care and ensuring access to care through legislative reform. Change in recent years has focused largely on preventative care and care for common medical conditions. However, health care after catastrophic injury, such as brain injury, is vastly more complicated.
Few individuals receive the full measure of treatment after brain injury that we now know will bring them to their ultimate recovery and functional status possible – due to uninformed financial restrictions to accessing care. We have learned that early treatment is better than late treatment, in part, because we can prevent the development of unnecessary complications. Expert treatment avoids inappropriate medications and surgeries while promoting and optimizing the neurological recovery of function.
“Patient-centered care” must be combined with the notion that “the dollars follow the patient” to enable this maximized recovery and return to the most meaningful and productive, as well as, the least expensive and least restrictive life after brain injury. Catastrophic brain injury presents unique challenges in comparison to other health conditions. A brain injury can affect multiple organ systems quite randomly, and it is often said that no two patients are the same. The tremendous variability requires medical treatment that is both comprehensive and expensive. Furthermore, the cost of treatment has not and will not be reduced to a pill or a surgery. So, treatment of brain injury requires a regiment of physicians, allied health professionals, case managers, attorneys, and family members, in addition to combination therapies that may also include surgeries and medications. Simply put, there is no medical condition today that is as complicated as brain injury.
Further, care pathways and endpoints of treatment are evident in most medical conditions. Appendicitis, as an example, is a medical condition that can almost always be treated the same way – but this is less the case for brain injury. Each patient recovers differently depending upon a host of variables that include the injury itself, the person’s educational, vocational and social history, the person’s pre-injury medical status, the person’s genetic factors, other system involvement, the timing of emergency treatment, the etiology of the injury, the expertise of the treatment given, the duration of treatment provided. Factors that affect access to treatment are also variables and may include access to insurance, socioeconomic status, patient and family education, and awareness of advocacy by treaters of appropriate treatment options.
What are the cost savings of a full-time comprehensive postacute rehabilitation program?
When treatment duration is determined by patient progress alone, rather than interference by financial restrictions, the data shows us that many patients seem to reach maximized recovery after injury when exposed to intensive and expert medical rehabilitation. These patients’ outcomes are stable or improving at extended follow-up 5 to 7 years post-injury. Additionally, the financial benefit to an insurance company or society is tremendous – at an average of $1.5 million per person lifetime. Incredibly, some patients’ recoveries have resulted in more than $7 million in lifetime savings. When the expense of these treatments is contrasted to the financial savings alone, the return on investment is truly immense.
Is access to health insurance vital for TBI recovery?
Health insurance is not yet routinely providing all the treatment one would reasonably prescribe in the first year after injury. This is not to say recovery doesn’t extend beyond this point in time; rather it says that this is the most rapid and easily modifiable recovery period. The solution is found in collaborating with the teams of professionals who work to determine how benefits are applied and medical researchers who are on the hunt for the most productive and efficient treatment. It is doubtful that recovery from brain injury will ever be reduced to a pill or a surgery. Recovery will remain dependent upon intensive, expensive and well-executed therapies combined with thoughtful use of appropriate medications and surgeries.
(Note: This is part one of a two-part series on issues affecting worker’s compensation, brain injury rehabilitation, and appropriate patient care).
The ultimate goal for the person with a traumatic brain injury (TBI) who participates in a comprehensive postacute rehabilitation program is to return to a productive life after discharge. Many times that involves returning to work. If the person sustained a brain injury in the workplace, he/she enters into the worker’s compensation continuum of care treatment system and is entitled to certain benefits that aim to reduce medical and living costs.
However, the public health care options available do not offer much in the way of treatment for TBI or stroke patients, as those options provide people with a considerably smaller chance at returning to higher productivity.
A collaborative report from the California Traumatic Brain Injury Advisory Board states, “For those significantly or profoundly impacted by this injury, reintegration into the community is overwhelming due, in part, to limited services and insurance coverage for critical medical and social rehabilitation. Moreover, persons with TBI often need help with community reintegration multiple times and at different junctures, because of the complexity of their injury and changes in their medical condition, living arrangement, or caregiving situation. (2010)” 1
Centre for Neuro Skills (CNS) has a legacy of success in the worker’s compensation industry and has helped thousands of people to return to productive lives. Since our inception in 1980, we’ve focused on community integration through an individualized, goal-oriented approach to therapy.
Postacute TBI rehabilitation that incorporates various therapeutic disciplines, including occupational therapy and vocational rehabilitation, can simulate real-world work environments, assisting people in re-learning skills for independent living. Through neurobehavioral therapy and behavior analysis in postacute care, clinicians can individualize the treatment needs of each person – increasing their participation in rehabilitation and community activities. This enables them to practice skills needed for independent living and provides them with a greater chance of a productive life post rehabilitation.
Can the benefits of postacute rehabilitation continue long-term?
A 2016 research study, led by Grace Griesbach, Ph.D., National Director of Clinical Research for CNS, investigated whether benefits of postacute rehabilitation for TBI are sustained after discharge from a full time comprehensive postacute rehabilitation program.
In the project, moderately to severely injured people with TBI who participated in a full-time comprehensive postacute rehabilitation program were interviewed one year after discharge. “In the analysis of employed and unemployed subjects, it was revealed that 43.75% had an occupation of equal position to that before an injury. Those that were working also showed positive levels for social participation, cognitive function, and social satisfaction,” the paper states. Additional analysis revealed that as many as 66% returned to some form of paid employment.
These findings support the durable outcome and beneficial effects of postacute TBI rehabilitation long-term, it noted, “concluding that individuals with a good rehabilitation outcome are more likely to regain their former occupation and quality of life.” 2
Do these findings also conclude that access to health insurance is vital for TBI recovery? I’ll address that topic in part two of this blog, Next Steps in Worker’s Compensation for Treating Brain Injury, which explores cost savings, reporting, data collection, and public health care options that are currently available.
Sources:
The usual course of medical interventions involves determining a diagnosis and an appropriate, relevant treatment. Once a determination is made, treatment options can be considered. Treatment options are developed over time and often, though not always, have a rigorous science behind them that serves to guide the implementation of that treatment. For example, an infection might be treated with one of several different antibiotics. The antibiotic selected must be the most potent drug for the bacterial infection – and it must be administered in a particular dose, a specific number of times per day, for a specific number of days. Additionally, a drug may come with advisories to avoid certain circumstances or other medications – for instance, a drug can cause increased sensitivity to the sun, and grapefruit juice can interfere with certain types of medication. Finally, few medicines are universally effective for all patients, and most can result in undesirable side effects.
There are very few drugs that have been explicitly developed for traumatic brain injury. In fact, rehabilitation is the most effective treatment known for reducing disability following traumatic brain injury. Little has been done to understand the dosing parameters similar to the manner in which medications are prescribed to represent the best use of rehabilitation.
In a research project completed at CNS, we were able to review the response to rehabilitation in nearly 400 people with traumatic brain injury. We found that response to treatment was different depending upon the severity of injury and time since the injury. People with mild to moderate levels of disability (who were more than one year since injury) showed improvements due to rehabilitation when treatment extended to 90 days or more. However, people with severe disability (who were more than one year since injury) required at least 180 days to show improvements.
People with either moderate or severe disability (who were less than one year since injury) showed improvement after 90 days of treatment – while those with severe disability showed even further improvement after 180 days of treatment.
These findings are important as they describe how people with different levels of disability also respond to a standard treatment intervention differently – both related to the severity of their disability and the elapsed time since their injury. Expectations for how long a person should be treated, what rehabilitation efforts should be, as well as cost, must be similarly adjusted. A “one size fits all” approach cannot be expected to result in a person achieving their highest level of recovery after a brain injury.
These findings argue for individualized dosing of rehabilitation following traumatic brain injury and, consequently, have implications for how payers and providers view application of rehabilitation following traumatic brain injury.
While there are no prerequisites for the job, parenthood is a lifelong responsibility. It is also one of the most fulfilling and important roles a person can have in life. Brain injury, unfortunately, impacts individuals without regard to their roles and responsibilities.
Persons with brain injury are challenged in their ability to care for themselves, much less others, making parenting more difficult. Yet, in order to achieve long-term success post-injury, family reintegration, including parenting, is imperative. And the best way to achieve this is through skill redevelopment during postacute rehabilitation.
The Basics Still Apply, Before and After Brain Injury
Parenting requires the ability to not only care for oneself, but to do so often in deference to caring for children. Parents are frequently required to subjugate their needs and wishes to the importance of providing for the well-being, nurturing, education, safety, development, and future of their children.
This requires a mindful approach, planning with a spouse or partner, or managing alone with family and friends to provide for housing, food, clothing, and education all the while seeking to instill family and societal values. Most parents want their children to be safe and to have a future that is the same as or better than their own.
Raising children presents a range of personal challenges to most parents. It may require developing a willingness for selflessness while acquiring skills as a teacher, mentor, role model, and disciplinarian, at least. Many couples acknowledge that arriving at a parenting style can be arduous and the source of conflict in their relationship as they negotiate stylistic differences and determine and articulate behavioral, educational, value, and moral expectations for their children.
Relearning Parenting Skills is Vital to Family Integration
After brain injury, however, individuals tend to become more focused on themselves, and fail to provide the same kind of parenting approach/skills as they exerted prior to injury. They are likely to be much less involved in child rearing, in general, failing to participate in determining, communicating, and facilitating goals for their children. These responsibilities either are not met well, or fall entirely to a non-injured spouse, partner, or family member.
Active discussions must be undertaken with an individual and/or couple to raise awareness of the importance of assessment and intervention for parenting skills, and to actively intervene to redevelop such skills and focus within the family. Family members must be relied upon to build an understanding of parenting skills and styles prior to injury as well as parenting-related family dynamics so as to serve as goals for treatment.
These efforts must focus not only on reacquisition of parenting styles and skills, but also on parental engagement with children in accordance with the manner in which they engaged prior to injury. Finally, teaching must include knowledge of common reactions children may have to the temporary or permanent loss of a parent to injury. Counseling can be extremely effective in raising awareness of these issues and changing behaviors within a family system. Counseling can incorporate other family members such as spouses/partners, children themselves, or key extended family members with meaningful insights such as close aunts/uncles or grandparents. Re-engagement within a family system to the various roles one played prior to injury is critical to the long-term success of family reintegration.
Individuals who sustain brain injury face a unique challenge with their health professionals. Brain injury is now widely viewed as a disease in the medical field, however patients are not yet granted the benefits and opportunities in treatment as are necessary for disease management. Increasing awareness of brain injury as a disease, and exploring the challenges of brain injury treatment will help us reevaluate our current system.
Brain Injury as a Disease
A brain injury is remarkably complex. Emerging evidence suggests that, like cancer, brain injury may actually be comprised of a number of distinct diseases that vary by the etiology of the injury, the nature of the injury, co-morbid health conditions prior to and since the injury, and factors such as gender, race, age, for example.
When the brain is injured, consequential effects often occur within immune, endocrine, and autonomic nervous systems’ functions. Persons with brain injury can become very sick, very quickly, seemingly only heralded by relatively minor early symptoms. Though we do not fully understand why this heightened period of illness occurs, it is likely a result, in some capacity, of the changes to the body’s systems’ functions.
Challenges of Brain Injury Treatment
Medical professionals working within the confines of our current system are often unable to dedicate sufficient time to a patient with brain injury in order to address the full scope of his or her injury, which includes cognitive, behavioral, communicative, and/or physical disabilities. Furthermore, these medical professionals are rarely able to stay current enough on the case to identify advisable and inadvisable medical practice patterns, thereby increasing the odds of treatment-induced complications.
Patients and their families cannot assume that medical providers are alike in their knowledge and experience. For example, the notion that patients can be best followed by practitioners in their home community is seriously flawed. Locality does not replace the prerequisite for a practitioner with expertise on brain injury. In fact, many of these less experienced practitioners are unaware of the comparative medical fragility associated with brain injury. Many poor medical decisions could have been avoided had the proper brain injury specialist been consulted.
Additional challenges can be found in the person’s inability to fully and competently participate in his or her medical care and decision-making. Cognitive, behavioral, communicative and physical disabilities following brain injury can make it difficult, if not impossible, for a person to recognize changes in his or her health, convey those changes, recognize improvements, or a lack thereof, in health following a medical treatment or intervention, accurately convey medical history or the history of present health problem(s), obtain appointments for procedures or laboratory studies, obtain prescribed medications or otherwise properly adhere to a prescribed treatment regimen. One might conclude that the attendance of an advocate or family member to medical appointments will mitigate such difficulties, and while helpful, such participation often fails to provide improved results.
Reevaluating our Current System
In my career, I have seen many downstream medical decisions result in serious and, sometimes, deadly consequences. These have always been avoidable and unnecessary, and borne out of a lack of knowledge.
A general physician cannot reasonably manage a patient with a complicated cancer, and brain injury is no different in this regard. We need to develop mechanisms that enable a patient with a brain injury all the same benefits as those allowed patients with complicated diseases such as cancer or cardiovascular disease. Simply put, there is no substitute for an individual case being followed closely by an experienced brain injury specialist.
Brain injury can change nearly everything, not only in the injured person’s life, but also within the lives of his or her family members.
Early after a brain injury, family systems become embroiled in the injury as they address arising issues. Sleep gives way to ICU vigils. Quiet moments give way to prayer. Casual discussions give way to serious conversation. These days are ruled by fear, with small glimmers of hope to serve as momentary relief.
Recovery, to a greater or lesser degree, eventually occurs. Time passes, hospital stays end, and the injured often return home.
Unfortunately, families are all too often solely responsible for redefining a new normal, as our society does not yet effectively provide sustained support. Understanding how to cope with the many changes after brain injury, and a willingness to implement coping mechanisms will make all the difference.
These eight tips are a great place to start:
Counseling can ease burdens and facilitate grieving, adjusting, and managing, all without giving up hope. However, not all families can afford such care, and for that reason, there are the other seven tips.
Realistic optimism, positivity, and hope offer an opportunity for a brighter and happier new normal. Humor can help keep spirits high. And in spiritually oriented families, solace and confidence come from actively practicing their faith.
Everyone handles grief and the subsequent changes within their lives differently. However, it is important to remember that each family member, no matter their role in the injured person’s life, is going through these changes together. Communication is a portal to common ground and unity.
Scheduling a regular time to discuss the injured person, and any related issues, can help family members to open up, creating a more approachable and manageable situation.
Imagine a wagon wheel with a hub and spokes. Families often operate by moving one member or another in and out of the center of the wheel, as his or her issues and needs call for priority. After a brain injury, it can become habitual to keep the injured person in the center of the wheel. It’s important for families to find a way to move others in and out of the circle again.
Taking care of oneself can seem inappropriate, especially for parents. However, if one uses oneself up in the care of others, there will come a time when the person has nothing left to offer others. Take time for yourself, and maintain some semblance of your hobbies and interests.
Because of the many demands of brain injury, it can be difficult to find the energy or money to socialize outside of the home. And it can feel wrong to seek pleasure while a family member with brain injury cannot do the same. Yet, socializing can help heal by providing a healthy sense of perspective.
Tell your friends what works, when you need to discuss the injury, and when you need to discuss anything but the injury. Friends and family may need your patience and forgiveness, as they may offer advice that is not useful or feels judgmental. No one knows how to act in these situations, and they are no exception.
7. When to Feel
There is time for grieving, sadness, and loss. So too, there must be time for hope, joy, and laughter. It is okay to take out the “pity pot” filled with your sorrow, despair, and loss. But then, with deliberation, put the “pity pot” back in the closet for another day. You will use it again and again, just always remember to put it away. In this way, you can avoid becoming mired in grief.
Some parents fear doing anything that might look or feel like they’ve accepted their child’s level of disability. It’s good to desire further growth and improvement post-injury, but there is a limit, and it is not healthy to be consumed by the drive to wring more recovery out of an injury. It is crucial to balance both acceptance of your new normal and hope for continued improvement.
One day I noticed the fine print on a cereal box, “Contents may settle during shipping.” The advisory served to avert any concern I might develop when opening the cereal to find it only three fourths full. I liken this advisory to balancing acceptance. So too will your “contents” settle as you move through your family’s changed world. One can and should actively explore changes wrought by brain injury in the family because realization of these changes will happen eventually, with or without your consent.
Those who find a way to bring balance back into their world are more apt to successfully take on the ripple effects of brain injury on their family dynamic. And, to be sure, the injured person will also flourish to the best of his or her ability in this normalizing and positive environment.
So, please make the decision to thrive. Be a light for you and your family. Find opportunities each day to laugh, dance, socialize, and communicate deeply. In this way, you can adjust to and manage in your new world.
Most people understand the important restorative value of sleep. However, the detrimental effects of sleep disorders are not as plainly understood and discussed.
Sleep disturbance is found in as many as 40% of individuals who have sustained a brain injury. Common sleep disorders include sleep apnea, difficulty falling asleep, difficulty staying asleep, difficulty awaking, and difficulty in achieving beneficial cycling between the various stages of sleep. This post will discuss a few key sleep disorders, the ramifications of sleep disorders, and proper and improper solutions.
Sleep Apnea
Snoring is the most obvious indication of sleep apnea, however snoring is not conclusive of sleep apnea. In fact, the only way to determine the presence of sleep apnea is through polysomnography (a sleep study). While there are devices that offer detection via headbands and other mechanisms, our research has shown that these devices are quite inaccurate and miss the majority of individuals with sleep apnea.
Sleep apnea has been linked to brain damage in heretofore healthy individuals. For a person who has already sustained a brain injury then, this link between sleep apnea and brain injury further emphasizes the drastic need for diagnosis and treatment.
Negative Effect: Growth Hormone Deficiency
Disruption of sleep at the wrong time in the sleep cycle may disallow the body’s production of growth hormone. If the body does not produce this important hormone in the early morning hours, it will not be available throughout the day. Exercise can help to increase the body’s production of growth hormone, however, this increase will not replace that produced in the early morning hours. Growth hormone deficiency leads to tremendous weight gain, high lipid levels in the blood, fragile bones, depression, cognitive problems, and, most importantly, real problems with the brain’s metabolism of oxygen and glucose (its two primary fuels). Growth hormone is extremely important to the brain’s ability to repair and maintain myelin, the insulating sheath that surrounds axons and impacts their speed of transmission and their plasticity.
Negative Effect: Memory
During normal sleep, particularly during REM cycles, information using large amounts of the brain’s resources is consolidated into more efficient holdings, and new information fuses with existing information. However, in those with sleep apnea and other sleep disorders, REM cycling is disrupted. This can negatively affect the brain’s ability to repair itself, ability to protect itself, memory function and metabolic efficiency. So, normalizing sleep is crucial.
Inefficiency of Medication as a Solution
Those who have difficulty falling and/or staying asleep may rely on over-the-counter sleep aids with or without medications that relieve pain. The drug (Benadryl or diphenhydramine hydrochloride) used in these over-the-counter agents actually can cause difficulty with memory, and a hangover effect the following day.
All medications used for sleep disturb REM cycling. As the importance of REM cycling was explained above, this consideration lends to suggest sleep aiding medications should be used with caution and infrequence.
Proper Solutions to Sleep Disorders
Good sleep hygiene is the most useful approach to overcoming many sleep disorders. This includes avoidance of caffeine; regular daily exercise before 7 PM; dark, cool, and quiet sleeping quarters; use of calming activities such as reading before bed; regular bedtime and wake time; and avoidance of waking to urinate or undertake other activities in the night. Alcohol consumption can result in awakening in the night as glucose levels in the blood drop, so alcohol should not be used to induce sleep.
After a brain injury, developing, guarding, and maintaining a routine of 7 to 9 hours uninterrupted sleep every night is critical. A good sleep study, use of an autoregulating BiPAP device for sleep apnea, daily exercise for 45-60 minutes, and good sleep hygiene are a good start to enhancing the body’s own abilities to heal, repair, and protect itself.
In 1977, Ed Breen of the Home Insurance Company identified a problem within the healthcare provisions for workers injured on the job. He approached a group of academics with a win-win solution, if it could be accomplished.
A number of individuals acquired catastrophic brain injuries in the scope of their employment with Mr. Breen’s company. Despite months of treatment in hospitals, these people were often left with tremendous levels of disability. Such disability translated to a very poor quality of life for the injured persons and their families, and a very high cost of continued care over the injured persons’ lifetimes.
Mr. Breen’s solution:
Reduce their levels of disability to an extent greater than that achieved at the hospitals, which leads to:
So, advances were made over the last 40 years in treatment of people who have sustained brain injuries through work-related incidents. Worker’s compensation professionals specifically designed an entire continuum of treatment to manage the catastrophic claims of their parent companies in concert with health professionals. Treatment was extended to rehabilitation in post-acute care; results spoke for themselves with many more people returning to higher levels of productivity and overall health, thus reducing long-term health costs.
Worker’s compensation has improved brain-injured persons’ level of care from what it was in 1977. I ask now, is that enough?
In California, the guidelines that are used by carriers and utilization reviews organizations are simple. They are presented from the Medical Treatment Utilization Schedule (MTUS) below in their entirety:
“Patient rehabilitation after traumatic brain injury is divided into two periods: acute and subacute. In the beginning of rehabilitation therapist evaluates patient’s functional status, later he uses methods and means of treatment, and evaluates effectiveness of rehabilitation. Early ambulation is very important for patients with coma. Therapy consists of prevention of complications, improvement of muscle force, and range of motions, balance, movement coordination, endurance and cognitive functions. Early rehabilitation is necessary for traumatic brain injury patients and use of therapy methods can help to regain lost functions and to come back to the society. (Colorado, 2005) (Brown, 2005) (Franckeviciute, 2005) (Driver, 2004) (Shiel, 2001)”
The above definition does not reference the continuum of treatment that has been used consistently over the last four decades. The continuum is shown below:
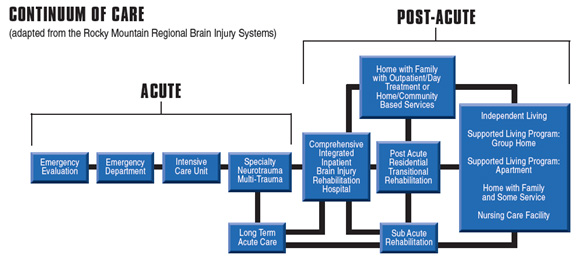
It is said that if “one has treated one person with a brain injury, they have treated one person with a brain injury.” That is to say, no two people who sustain a brain injury are alike. Brain injury is one of the most, if not the most, complicated medical conditions to be encountered. And, brain injury is often accompanied by other system injury or involvement.
Not only is brain injury tremendously complex, but so must be treatment for brain injury. The above continuum provides for numerous treatment setting options, each with distinct dosing advantages for specific subgroups of patients who are experiencing unique constellations of deficits following brain injury. These deficits can include medical, physical, communicative, cognitive, psychological, and/or behavioral disorders requiring careful selection of the treatment setting most likely to properly dose treatment of the problems presented by any given individual.
So, why does the State of California operate under such simplistic guidelines? Is this the best we can do?
One solution may be to adopt other guidelines that have far better information to offer pertaining to brain injury. Two of these include the Colorado Medical Treatment Guidelines (2012) and the Official Disability Guidelines.